Cat. No.: 514 003
Amount: 50 µg
Price:
$380.00
|
|
|
|
| Cat. No. 514 003 |
50 µg specific antibody, lyophilized. Affinity purified with the immunogen. Albumin and azide were added for stabilization. For reconstitution add 50 µl H2O to get a 1mg/ml solution in PBS. Then aliquot and store at -20°C to -80°C until use. Antibodies should be stored at +4°C when still lyophilized. Do not freeze! |
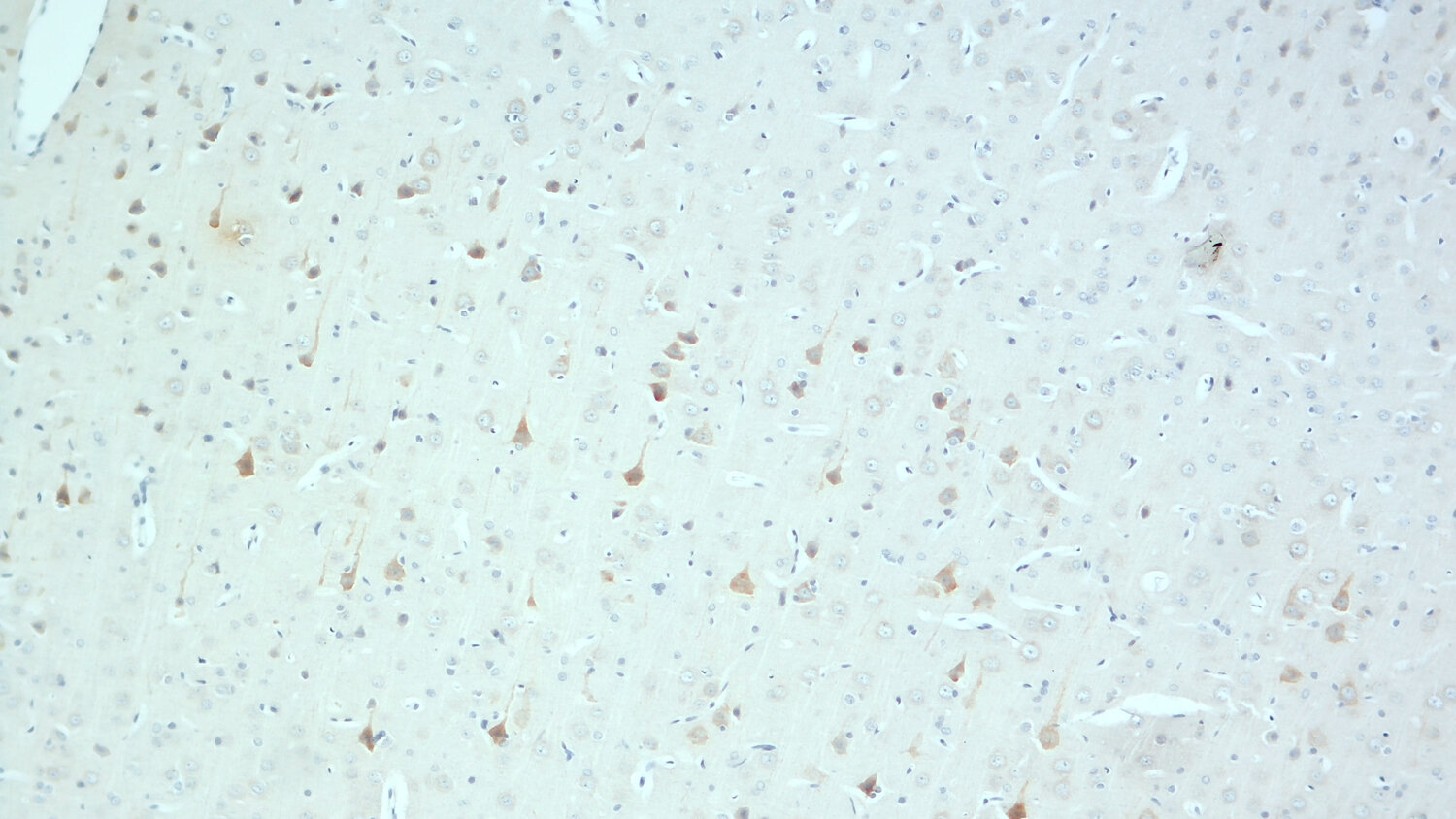
| Applications | |
| Immunogen | Synthetic peptide corresponding to AA 58 to 85 from mouse GIP (UniProt Id: P48756) |
| Reactivity |
Reacts with: mouse (P48756), rat (Q06145). Other species not tested yet. |
| Specificity | The antibody is specific for GIP. It may show minor cross-reactivity to related peptide hormones. |
| Data sheet | Datasheet 514_003 |
|
|

Gastric inhibitory polypeptide (GIP), also known as glucose-dependent insulinotropic polypeptide, is a member of the secretin/glucagon superfamily of peptides. It is a well conserved 42 amino acid peptide generated by post-translational cleavage of the precursor protein proGIP (1).
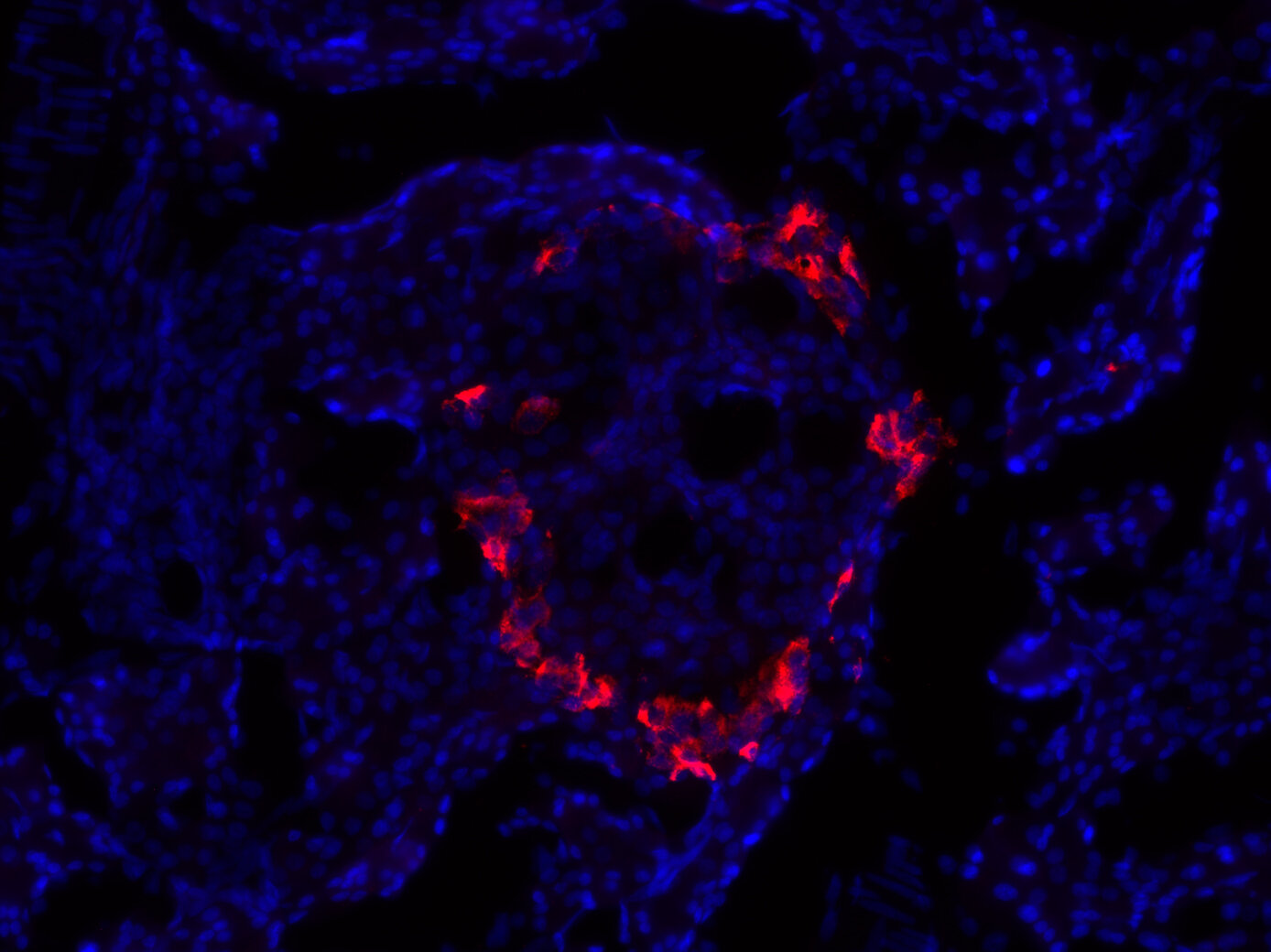
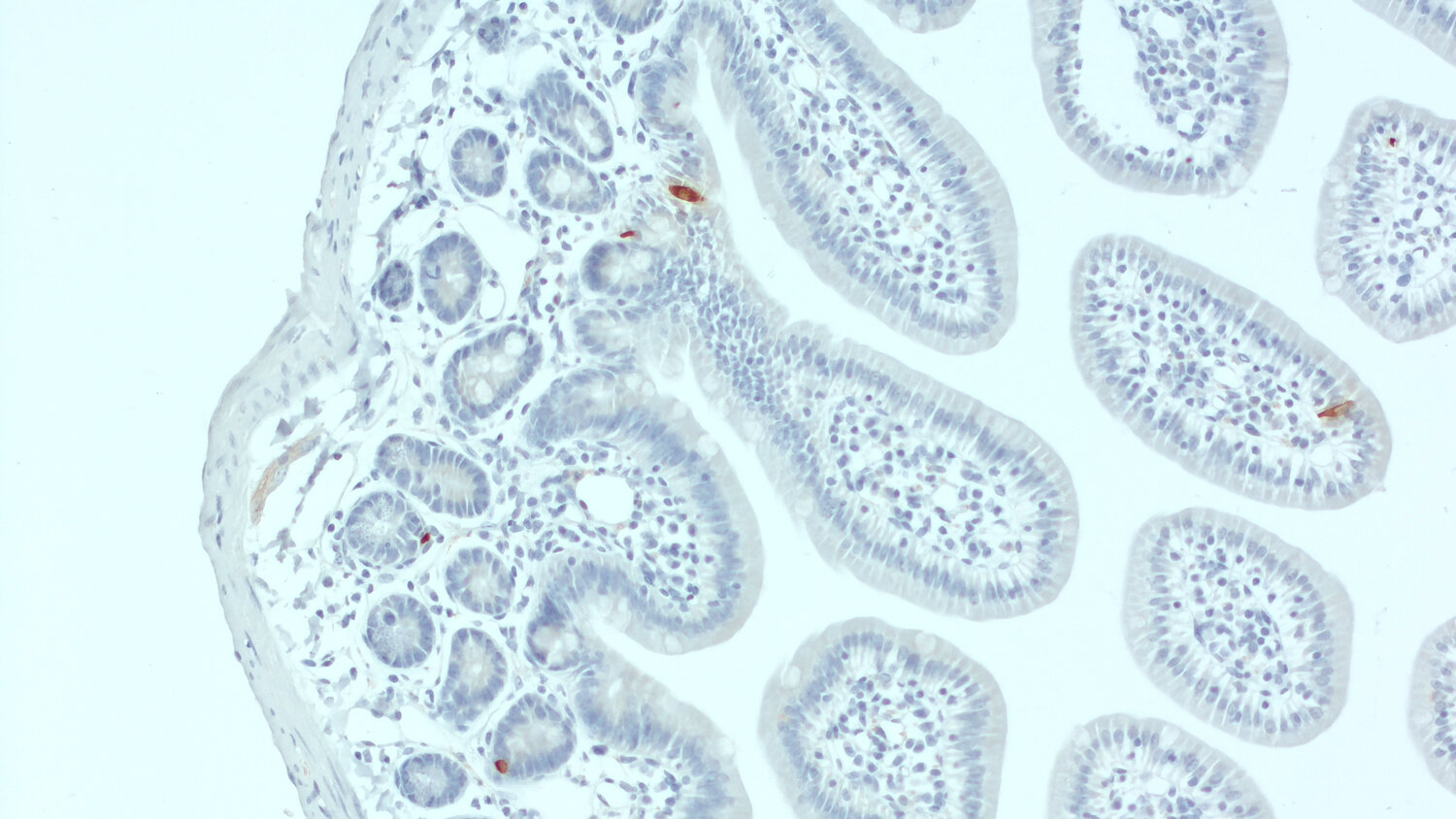
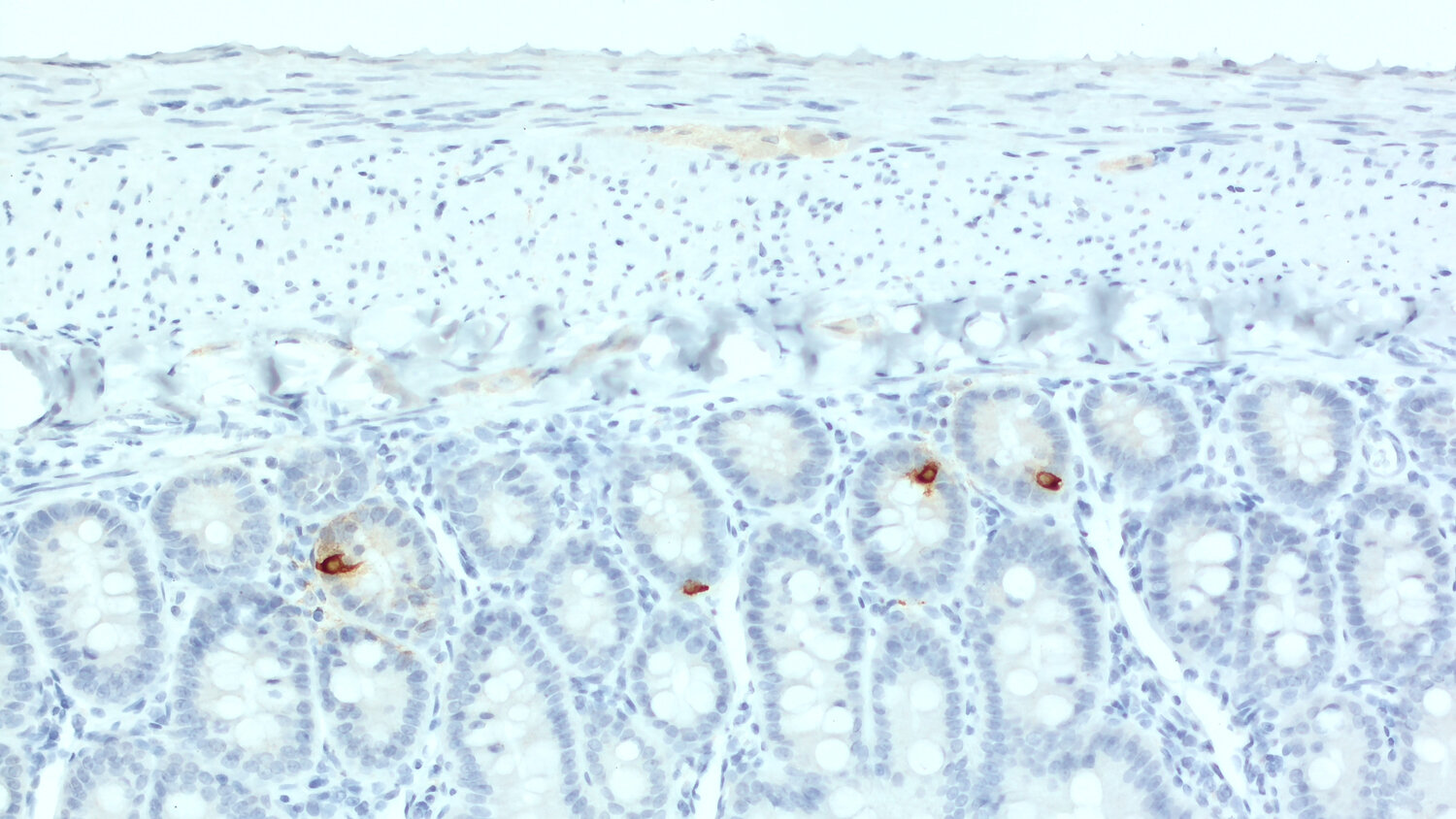
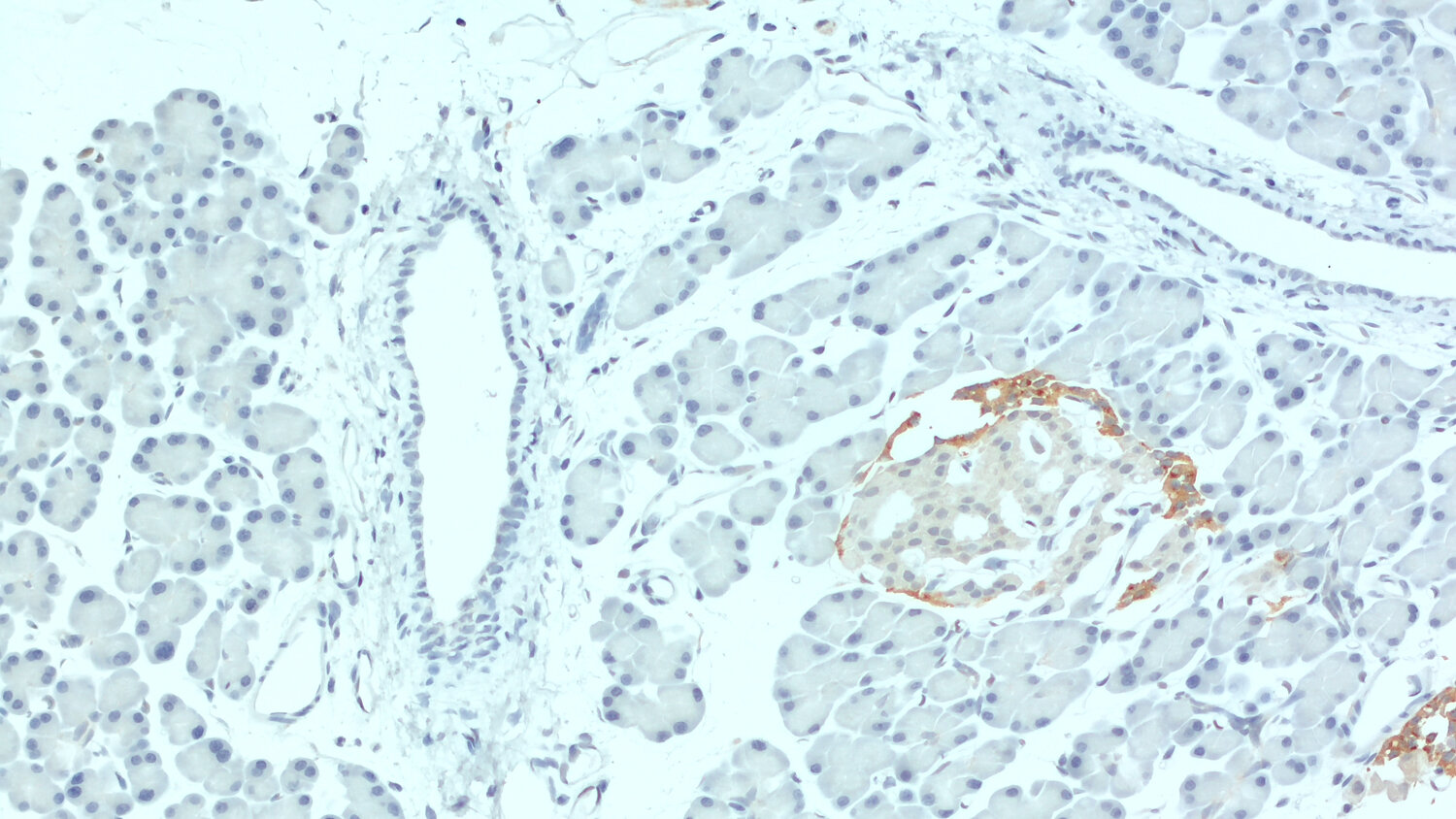
GIP is synthesized by enteroendocrine K cells of the small intestine, found in highest concentration in the duodenum. It is released into the circulation in response to glucose or fat ingestion (1). A short but bioactive form of GIP (GIP1-30) is secreted from pancreatic alpha-cells within the pancreatic islets (2). In the CNS, GIP is expressed in several brain regions including the cerebral cortex, hippocampus, and olfactory bulb (3).
GIP exerts its effects via interaction with its G-protein-coupled receptor. In pancreatic beta-cells, it increases adenylyl cyclase activity, thereby stimulating insulin secretion (1,2). GIP is also implicated in the control of lipid metabolism and the development of obesity. In adipose tissue, it increases lipoprotein lipase activity and lipogenesis (1,4). Recently, GIP appeared as a major player in bone metabolism and bone cell physiology by preserving bone strength (4,5). In the brain, GIP induces neuronal progenitor cell proliferation and has a neuroprotective function (3).
Certificates
ISO 9001 2015 Quality Management System and Green Lab Platinum certification level for sustaining laboratory processes.


Newsletter
Sign up for our newsletter and get the latest updates and news.